
What is Myopia?

Myopia, or short-sightedness, is a condition where distant objects appear blurred because the eye focuses light in front of the retina instead of directly on it. A child or adult with myopia sees clearly up close but struggles with distance vision, and usually needs control lenses or spectacles to correct it. In Singapore, myopia is one of the most common vision conditions in children, which is why early detection and myopia control matter.
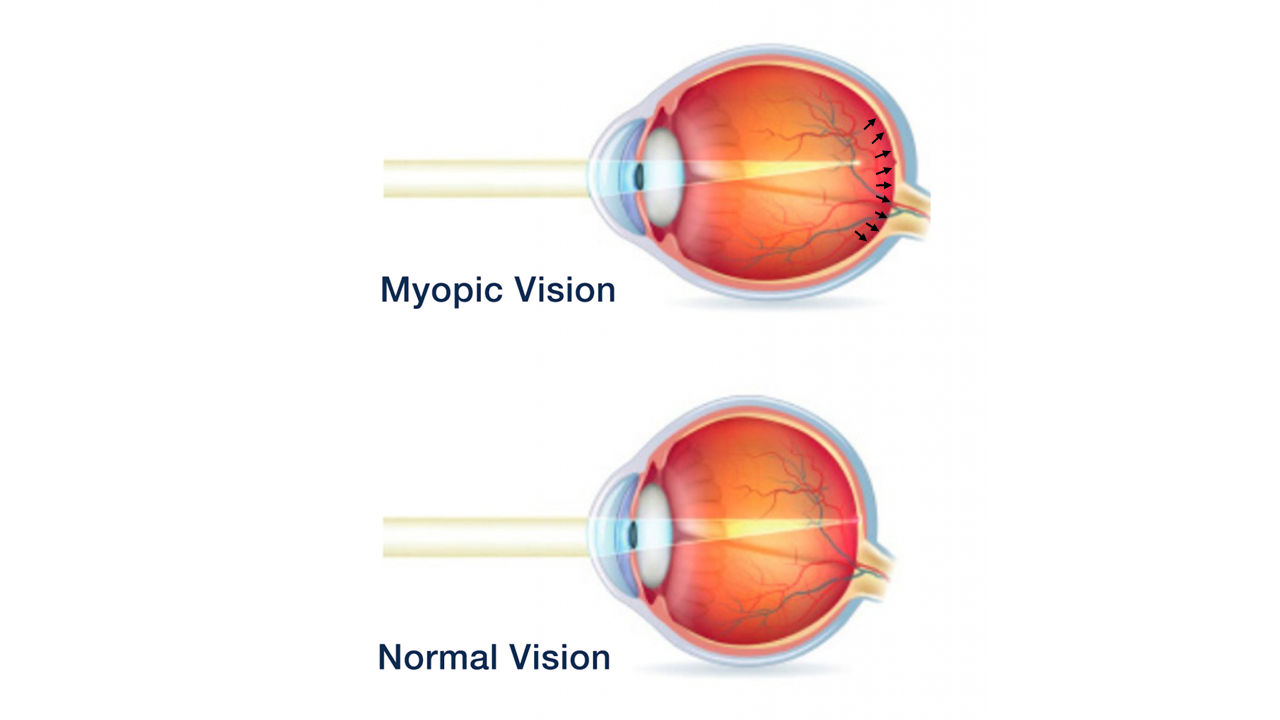
The myopic eye
Myopia develops when the normal growth of the eyeball is disrupted. The myopic eye is elongated — stretched longer than it should be — so light from distant objects focuses in front of the retina rather than on it, causing blurred distance vision.
The normal eye
In a normally developing eye, the structures grow in unison so light focuses precisely on the retina at the back of the eye. Vision is sharpest when light lands exactly on this retinal plane — how the eye is naturally programmed to grow.
What causes myopia in children?
Both genetics and environment contribute to the development of myopia in children and teenagers. A family history of short-sightedness significantly raises a child's risk. Environmental factors include excessive near work, reading, studying, screen and tablet use, and time spent indoors.
Significant eye growth happens between ages 6 and 12. During this critical window, anything that drives abnormal elongation of the eye increases myopia. As urbanisation, academic demands and screen time have risen, childhood myopia in Singapore and worldwide has climbed sharply — so much so that researchers now call it the myopia epidemic. The encouraging news is that with early intervention, the severity of myopia through childhood can be managed.
Degrees of myopia
Myopia is graded by the strength of the prescription lens needed to correct vision, measured in dioptres (D). The higher the myopia, the greater the physical elongation of the eye.
- Low myopia: -0.50 to -3.00
- Moderate myopia: -3.25 to -5.75
- High myopia: -6.00 and above
- Extreme myopia: sometimes used for myopia beyond -10.00
In Singapore and across Southeast Asia, myopia is often described in "degrees" — for example, -6.00 is commonly referred to as 600 degrees (600 度近視). Accredited optometrists in Singapore typically measure in dioptres.
Why childhood myopia is worth controlling early
Myopia is more than the inconvenience of needing glasses or contact lenses. Because the myopic eye is physically stretched, the retina becomes thinner — like an over-stretched elastic band — and more vulnerable to damage and disease. There is no "safe" level of myopia, but the higher it climbs, the greater the lifetime risk of sight-threatening conditions.
Consequences of high myopia
High myopia can be managed with several treatment options, but it still carries serious long-term health risks:
- Thicker lenses — glasses become heavier, and high-index lenses add cost with each new pair.
- Cataract — associated with earlier formation and higher surgical risk.
- Glaucoma — linked to a higher incidence and more severe cases.
- Floaters — earlier vitreous detachment causes more visual floaters and glare.
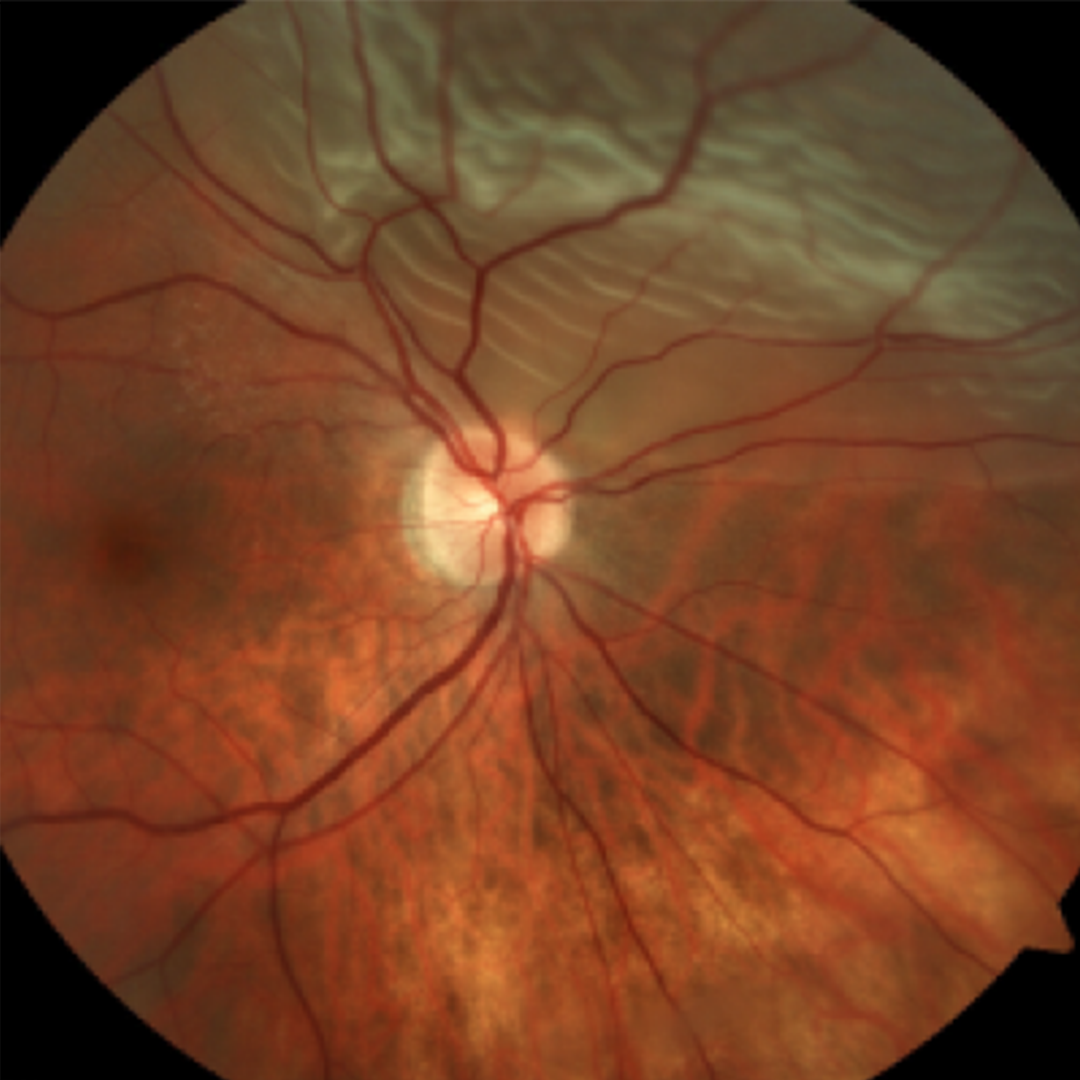
- Myopic macular degeneration — retinal thinning can lead to loss of central vision.
- Retinal detachment — a small retinal tear can progress to detachment and permanent vision loss if not treated promptly.
Symptoms of retinal detachment can include flashes of light, a sudden increase in floaters, or a shadow moving across your field of vision — all of which need urgent assessment.
What causes myopia in children?
Both genetics and environment cause myopia. Genetics and environmental factors together contribute to the development of myopia in children and adolescents.
A family history of myopia is a known risk — one or both parents being short-sighted significantly increases a child's chance of developing it too.
Environmental influences include excessive near work, reading, studying, computer and tablet use, and time spent indoors. Significant growth of the eye occurs between ages 6 and 12, and during this critical window any factor that drives abnormal elongation of the eye can result in myopia.
As society has urbanised — with heavier education demands and constant digital technology from a young age — the human eye hasn't kept pace with these rapid changes. That's why childhood myopia is rising dramatically, not just in Singapore but globally, to the point that researchers now call it the myopia epidemic.
The encouraging news: with early intervention and myopia control, it is possible to lessen and manage the severity of myopia through childhood and adolescence.
Degrees of myopia
Myopia is classified by its degree — the power of the prescription control lens needed to correct the blurred vision, measured in dioptres (D). The higher the myopia, the greater the physical elongation of the eye.
- Low myopia: -0.50 to -3.00
- Moderate myopia: -3.25 to -5.75
- High myopia: -6.00 and above
- Extreme myopia: sometimes used to describe myopia beyond -10.00
In some countries, myopia is described in "degrees." In Hong Kong and Southeast Asia, -6.00 is commonly called 600 degrees of myopia (600 度近視) and -10.00 is 1000 degrees (1000 度近視). Accredited optometrists and opticians in Singapore usually measure in dioptres, though many Singaporeans still refer to their spectacles or control lenses using the "degrees" descriptor.
The dangers of myopia
Myopia is far more than the inconvenience of relying on control spectacles or contact lenses to see — it is a real danger to the long-term health of the eyes.
Glasses and contact lenses correct vision by refocusing light onto the retina, but they don't address the underlying problem: the eye is physically stretched and elongated. That means the retina is thinner — think of an over-stretched elastic band — and more prone to damage and disease.
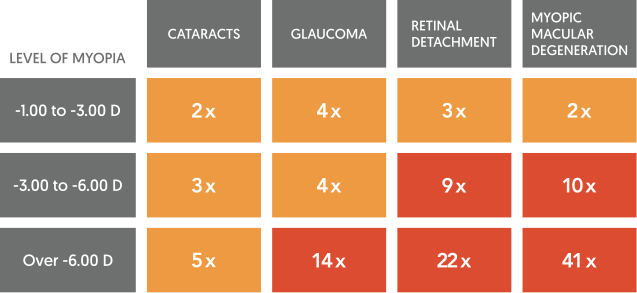
Some of the potential consequences of high myopia are detailed below. There is no "safe" level of myopia — even moderate myopia can have consequences — but the higher the myopia, the greater the danger of vision loss across a person's lifetime.

CONSEQUENCES OF HIGH MYOPIA
While high myopia can be managed through several common treatment options, it still poses high health risks that can severely impact quality of life over time.

Glasses become thicker and heavier with higher levels of myopia. High-index spectacle lenses to reduce thickness also add extra expense to each pair of new glasses.
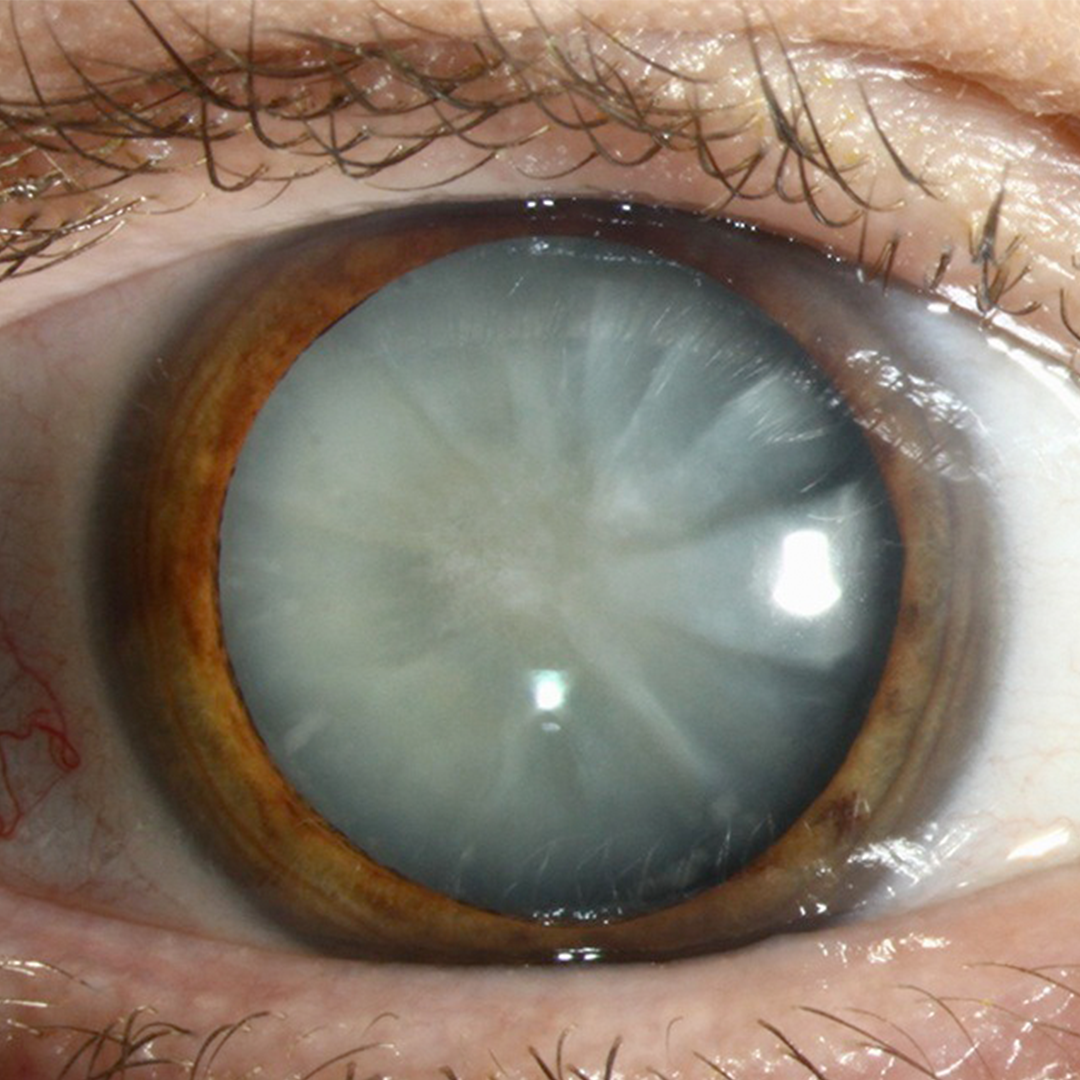
High myopia is associated with cataract formation, and also increases the risk of complications during and after cataract surgery.

High myopia has been linked to a higher incidence of glaucoma, and development of more severe cases of glaucoma.

Myopia commonly causes earlier vitreous detachment, leading to many visually-disruptive spots and floaters and increases glare.

Thinning of the retina in a highly myopic eye increases the risk of developing myopic macular degeneration, causing loss of central vision.
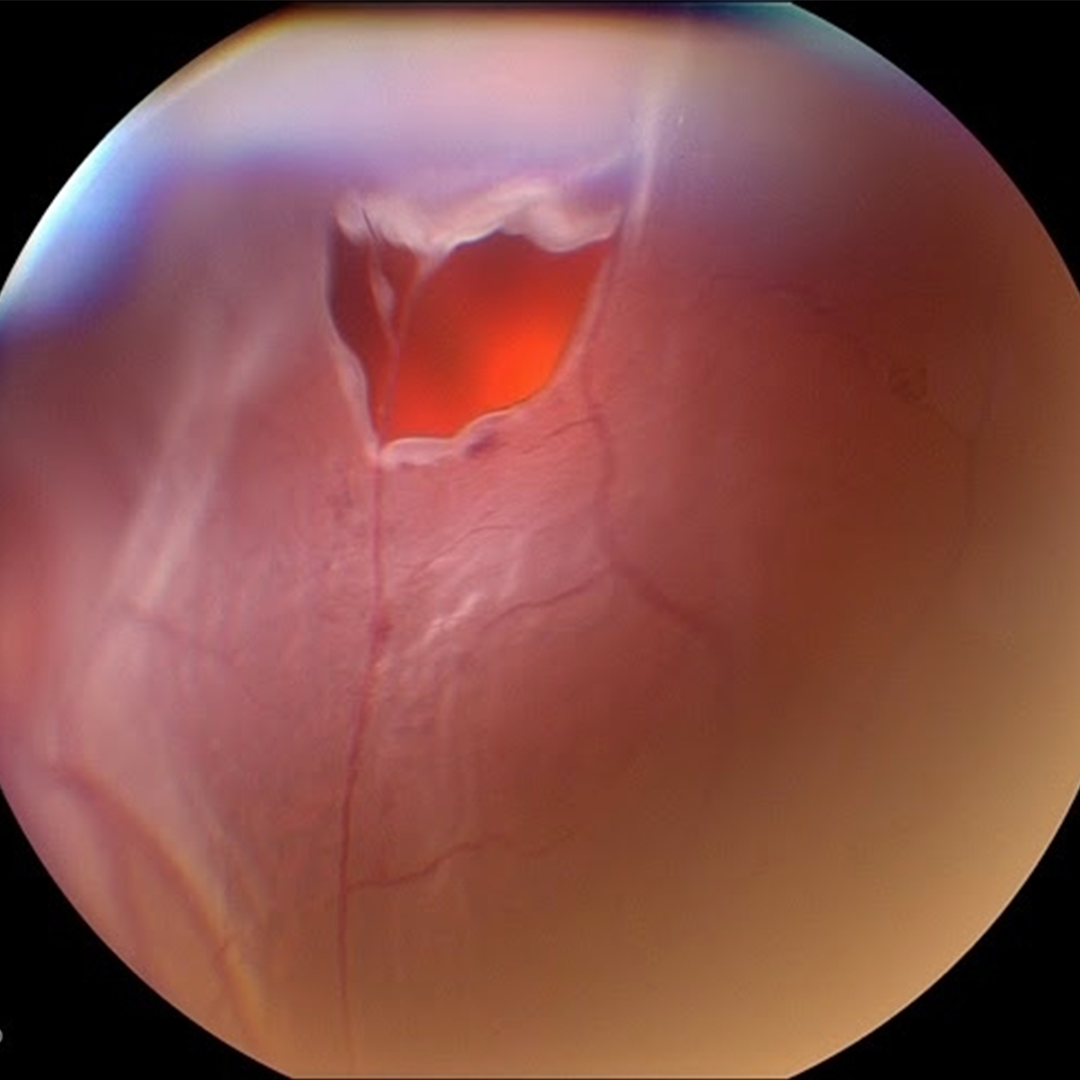
A small tear in the retina can quickly develop into a retinal detachment, which, if not detected and managed promptly, can lead to permanent vision loss.
Symptoms of a retinal detachment may include flashes of light, sudden increase of floaters, and a large shadow moving across the line of sight.
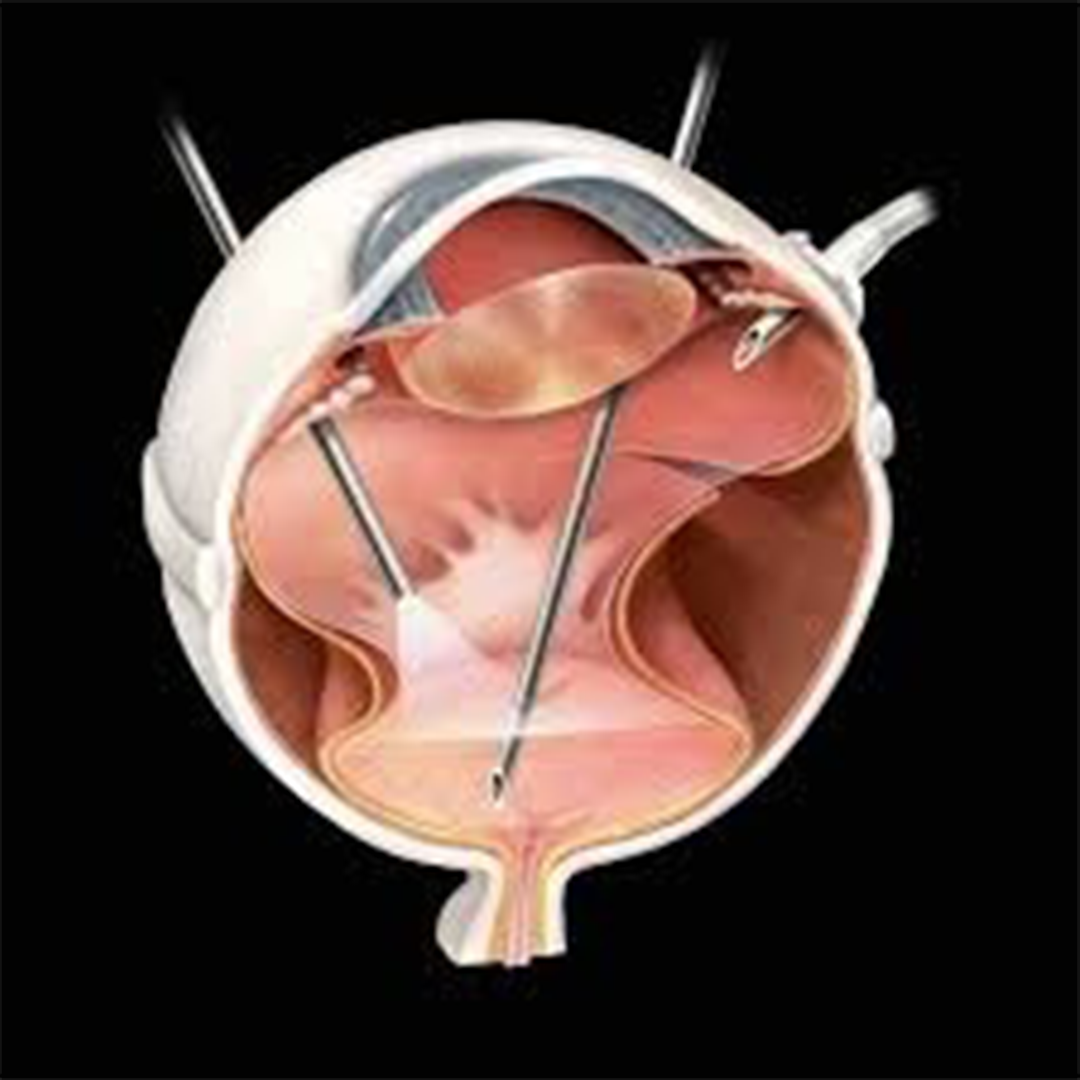
Retinal detachment surgery to repair a torn retina and restore sight is a complex, risky and invasive procedure. Vision may never fully return to normal.
Myopia is irreversible
The Myopia Epidemic in Singapore and Worldwide


The myopia epidemic in Singapore and worldwide
Myopia is rising globally at an unprecedented rate, and Singapore has one of the highest childhood myopia rates in the world. More than 80% of teenagers and young adults across East Asian populations — Singapore, Hong Kong, China, Taiwan and Korea — are short-sighted, with some groups now exceeding 90%.
Myopia is no longer only an Asian problem. The number of young people with myopia outside Asia — across Australia, the United States and Europe — has doubled in a single generation and continues to rise. Projections suggest around half the global population could be myopic by 2050.
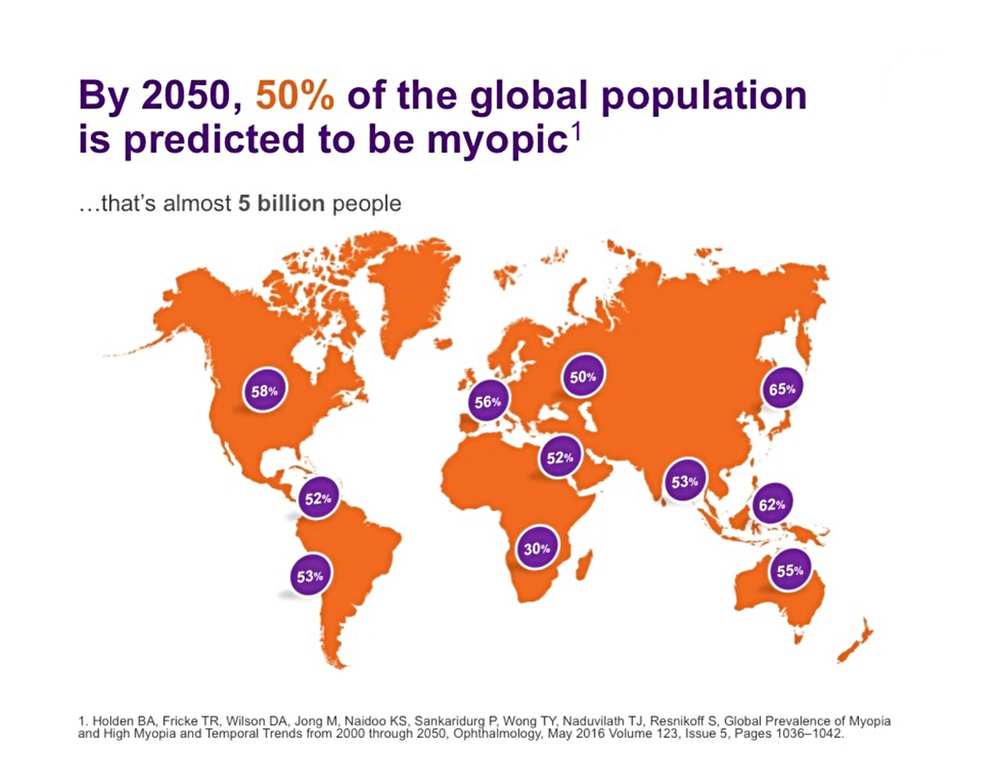
The World Health Organization's 2016 report on myopia warned that myopia and high myopia are increasing worldwide at an alarming rate, raising the risk of vision impairment from conditions such as retinal damage, cataract and glaucoma.
— Summarised from the WHO Report on Myopia, 2016
What's driving childhood myopia?
Genetics. A child with one myopic parent has roughly three times the risk of developing myopia; with two myopic parents, around six times the risk. As myopic children become myopic adults, the prevalence compounds across generations.
Environment. Children today use digital devices far earlier and for longer than previous generations. Education in Singapore is demanding and screen-heavy, while higher-density living means less outdoor time and more close-up indoor activity — all contributing to the myopia epidemic.
Slowing Down Myopia: A Proactive Approach
Slowing down myopia: a proactive approach
Myopia control is a set of evidence-based treatments that slow how quickly a child's short-sightedness progresses, reducing their lifetime risk of high myopia and related eye disease. Many optometrists simply update a child's glasses each year as their myopia worsens — at EMME Visioncare, our MyopiaControl programme takes a proactive approach to slow that progression.

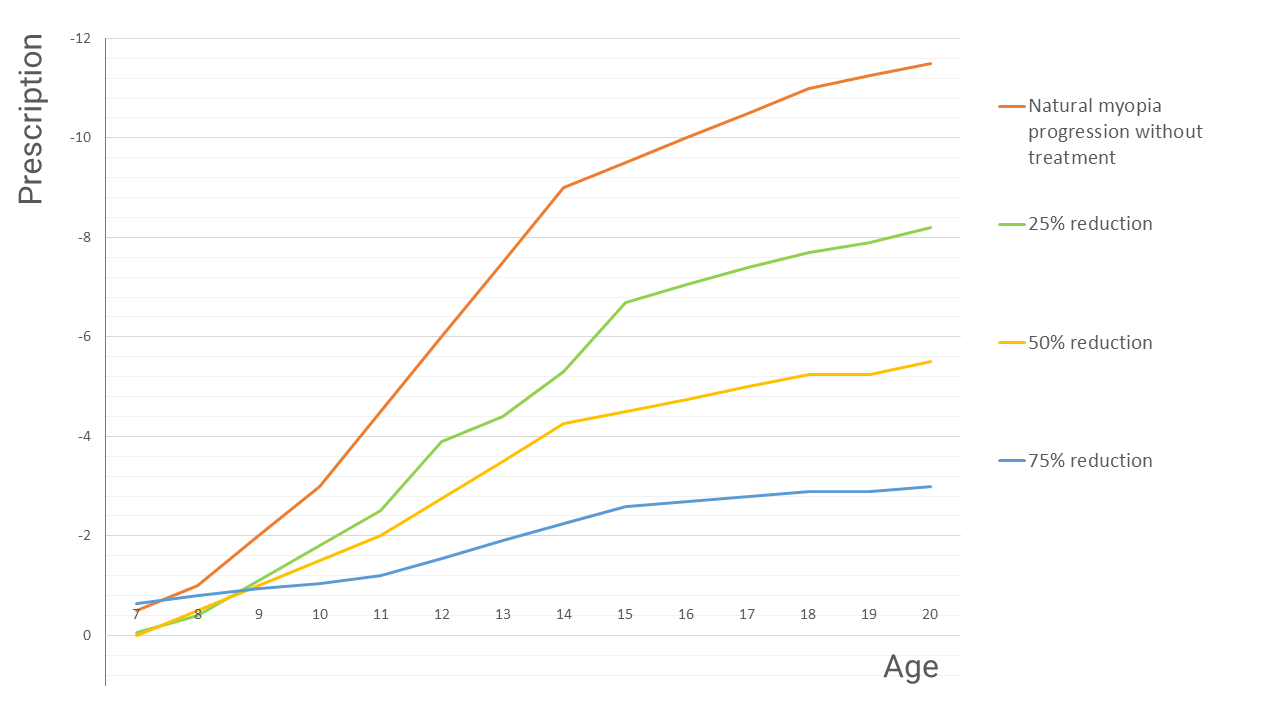
By prescribing treatments that delay onset and slow the rate of progression in short-sighted children and teenagers, we lower the risk of myopia-related vision loss later in life. Published research shows suitable children can slow progression by around 25–75% (an average reduction of roughly 50%) — a meaningful difference to a child's long-term eye health.
How does myopia control work?
Myopia typically progresses when the eyeball grows too quickly between ages 6 and 12, stretching the eye in length. Research suggests the peripheral retina sends signals that drive this growth. When peripheral light signals are altered — by modifying the optics of a corrective lens, or by reshaping the eye surface with orthokeratology — those growth signals are reduced, slowing myopia progression.
When should myopia control start?
As soon as significant progression is documented. We review children with myopia every 3 to 6 months and assess their risk based on age, current myopia, history, and genetic and environmental factors. A documented increase of -1.00D or more in a year (or over two review visits) is considered significant progression and a trigger to begin treatment.
There is no minimum age to start. Suitable treatment types may vary with age, but earlier intervention generally leads to a better long-term outcome. Each year of delay during rapid progression can make a real difference to whether a child eventually develops high myopia.
The goal is to avoid high myopia. Keeping a child's myopia as low as possible reduces the lifetime risk of glaucoma, retinal detachment and myopic macular degeneration. While there is no "safe" level of short-sightedness, prevention is far better than cure.
Myopia Control Solutions in Singapore
There are several proven myopia control options, and the right choice depends on your child — their age, prescription, rate of progression and lifestyle. At EMME Visioncare, our optometrist begins with a detailed assessment of your child's eyes and eyesight history, then recommends an individualised treatment plan. We graph prescription changes over time to track progression and adjust the plan for the best control.
![]()
1. Orthokeratology (Ortho-K)
Orthokeratology is among the most effective optical treatments for myopia control. Ortho-K lenses are custom rigid lenses worn during sleep that gently reshape the cornea overnight, giving clear daytime vision without glasses while slowing myopia progression. They suit children with rapidly increasing myopia, typically between -1.00 and -6.00. Reversible, safe and non-invasive, Ortho-K is often described as braces for the eyes.

2. Myopia control soft contact lenses
Dual-focus soft contact lenses use special peripheral optics to slow eye growth. At EMME Visioncare we fit the CooperVision MiSight 1 Day myopia control lens — a daily disposable worn during waking hours, comfortable and well suited to children with milder progression or those not yet ready for Ortho-K. Ordinary soft contact lenses do not provide a myopia control effect.
3. Myopia control spectacle lenses
Modern myopia control spectacle lenses use peripheral-defocus optics — a clear central zone for sharp vision, surrounded by treatment zones that signal the eye to slow its growth. They are worn just like ordinary glasses, with nothing to insert, making them a practical option for many children. We fit three clinically studied defocus designs:
- HOYA MiYOSMART — D.I.M.S. technology, with long-term clinical follow-up data.
- Essilor Stellest 2.0 — H.A.L.T. MAX technology, with a clinical trial conducted in Singapore.
- ZEISS MyoCare — ZEISS's defocus spectacle lens for managing childhood myopia.
Older multifocal and bifocal designs may still help children who are less suited to contact lenses or atropine; these incorporate a reading power to ease focusing demand during near work. Ordinary single-vision lenses provide no myopia control effect.

4. Atropine eye drops
Low-dose atropine is a medical myopia control treatment, applied as a single drop in each eye before sleep while the child continues to wear their usual correction by day. A very low 0.01% concentration is used; clinical trials in children show little to no side effects at this dosage, and it is considered safe for long-term use. Our optometrist co-manages this treatment with an ophthalmologist, who prescribes and dispenses the drops.

5. Lifestyle changes
Simple habits support myopia control, though they don't replace clinical treatment:
- Spend at least 90 minutes outdoors each day
- Take a 5-minute break every 30 minutes on screens
- Limit smartphone and tablet time
- Keep at least an elbow's distance from the page and read under good lighting
- Maintain good posture for reading and writing
Not sure which option is right for your child? Book a myopia assessment and our optometrists will recommend a tailored plan.
Our Evidence-Based Approach to Myopia Control
At EMME Visioncare, our MyopiaControl treatment strategies are based on published, peer-reviewed research and current international clinical approaches to controlling myopia progression in children. As the science advances, we update our strategies so the children we care for receive current, effective myopia control.
Selected published research on current myopia control treatments:
A note on undercorrection
Some parents believe a weaker prescription — or no glasses — will "preserve" a child's eyesight. Current evidence shows the opposite: undercorrecting myopia, or going without needed correction, may actually accelerate progression because of the effect of blurred vision on eye growth. For this reason we do not prescribe undercorrection for myopic children.
Everything we recommend is grounded in research, and we're happy to share it with you. Book an appointment to start your child's myopia assessment.